Ashwagandha’s effect on bipolar disorder

Overview
- Anecdotal Story
- Ashwagandha’s Effect on inflammation
- Bipolar Disorder And The Divided Self
- Bipolar Disorder Most Common Comorbidities And How Ashwagandha Can Help
- Real Talk
- Denial
- Conclusion
- References
Ashwagandha’s Effect On Bipolar Disorder An Anecdotal Antidote
When I first heard about Ashwagandha, I was 19 years old and struggling to stay active, looking for a vitamin to help with stress and fatigue. I will admit that I was surprised at how well it worked. Not only for stress and fatigue, but I was also noticing some other positive effects when it came to physical health, specifically with my joint health. The following is a first person account of trying Ashwagandha for the first time. Unfortunately i had a hypomanic episode during my first couple of weeks so the first person account will be explained further in this article.
I know that inflammation after a hard workout is to be expected, but is joint pain? This is something I have asked myself many times. Even at a young age, my joints would feel hot and stiff. Granted, I was overweight but relatively young, about 14 years old. And it’s not uncommon for people who are obese to suffer from joint pain because they tend to live a sedentary lifestyle (which I had) and have added stress on their joints. But at the age of 19, I had finally managed to lose over 100 pounds and was at 220 pounds, a healthy weight for a 6 foot male, but I had not managed to lose the joint pain. So what gives? Do I have arthritis? What’s causing this inflammation? Is it my workout habits? Questions like this gnawed at me. I would lay awake in bed in discomfort, trying to heal after a workout that day but not being able to fall asleep and recover. The pain would come and go. I didn’t make a big deal about it at the time, as I thought it was something everyone went through. Fast forward a couple of weeks, and I decided to try Ashwagandha after doing some reading on the effects on mood and overall health, I thought it would be a nice boost of energy for working out, unaware of the full potential this herb had.
The first week, I definitely noticed a difference in my mood, energy, and body. It took me a week before I realized that my joint pain was no longer bothering me. My sleep improved, and I felt rejuvenated, but for how long? I thought to myself. It’s no secret that the body can build up a tolerance to supplements and some medicines. for example, L-theanine is a supplement used for anxiety, but many people experience a tolerance build up just after 5 days. You then need to wait about 10 days before your tolerance goes back to baseline. The thought of this tolerance build up worried me; at this age, I was sick and confused with my mental and physical health and was looking for some stability. I had the mind of a hypochondriac, but for good reason, I had a suspicion that I was not like the rest of my friends or the people around me. Patterns of behavior made me feel like I was unstable in my sense of self.
Around this time I was seeing a psychiatrist, but like many young Americans who are confused as to what they are feeling, exhibiting signs of anxiety is a normal reaction to the unknown. Psychiatrists are able to see patients for 10 to 20 minutes (at least mine did), which is enough to take a snapshot of the patient’s emotions and state of mind. So it was not so surprising that I got prescribed fluoxetine (A common medication for anxiety)for my first visit. I wanted to tell my psychiatrist more, because it felt like there was something else at the root of the problem, but I didn’t know how to explain and part of me didn’t want to know.
Hypochondriac. That word… that prickly word, like a jumping cactus, was flung and impelled at the back of my mind after my first visit to the psychiatrist. Maybe it really is all anxiety. Ever since I was in high school, I was afraid of having bipolar disorder or even borderline personality disorder, but trying to give a reason to the doctor on why I thought this felt impossible. My brain gets scattered and compartmentalized, so I gave up on trying to understand and took the medicine, hoping time would prove me wrong.
Upswing
7 weeks past after that first psychiatrist visit before i decided to give Ashwagandha a try. And now 2 weeks into taking Ashwagandha i found myself feeling good………really good, like too good. Like, I can do anything type of “good” I feel like I can push myself to my absolute limit! I want to run, jump, scream. Wait. Is this the Ashwagandha that’s causing me to feel this good? Or maybe the fluoxetine? Maybe both!? There are so many pieces to the puzzle that I can’t piece them all together. My mind was racing. How do I begin to explain with all the variables?
Lost in my own head, in a sea of doubt, swimming and looking answers. My limbs fall asleep, too numb to feel myself or the outside world. I am hoping am not off the deep end as I search for footing, but I know I am sinking; I am at the mercy of the waves.
I feel as if I could do anything, but at the same time, I don’t feel in control. I have all the energy I need, and I feel amazing, so who cares? Why worry? Why argue with myself? So I decided to work out at home, wanting to take advantage of this familiar feeling. I could feel a storm of adrenaline and endorphins approaching me, and with arms outstretched, I embraced the downpour. I felt unstoppable, insatiable, I wanted a fight….. but this weak body, I thought to myself; I have the spirit and the energy, but my tools are failing me. I remember feeling my tendons stretching and locking in place, forcing knots to form in my calves, my hamstrings shaking under the tension. My lower back felt like it was collapsing into itself. Each irregular heartbeat made me more and more irritated that my body could not keep up. I don’t remember what I was doing specifically for my workout, but I don’t think that matters in getting the point across. I was in pain, and I felt alive and powerful.
“All these hormones, and yet……. and yet they are mostly useless now. They are now considered a nuisance for the way they make us feel. We have all this power fitted for an old world that people are too good for ” I said to myself, panting out of breath with my head up high and my body erect, ready to die fighting. I remember thinking back to documentaries about how people used to live in the wild, fighting to survive. In my manic state I felt as though I had tapped into some sort of ancestral primal gift that is inside of us all. I could feel my scalp tingle as my ego inflated, my mind exterminating any negative thoughts I had about myself.
I was high, high off my own supply, not from fluoxetine not from Ashwagandha but from my own brain chemistry. This feeling, this is who i am, this is how I am meant to be, this is what confidence is and I never want to let it go.
Thinking back to this thought depresses me because that wasn’t fully me. I was on my way to having a hypomanic episode, something that happens to people with bipolar disorder type 2 and 1. Part of me disintegrates, and I am no longer whole. Grandiosity starts to rot away my perception. Thoughts no longer have the same meaning as they used to. My mood had shifted, and it felt as though I was no longer the same person. This feeling felt so freeing, but I felt guilty. I laughed. I cried. my thoughts felt like they were harassing me. I was tired of this feeling; I shouldn’t be feeling like this. It doesn’t make any sense.
“Guilt? , you feel guilty? For what? being happy? What’s wrong with that? Let’s keep going, ignore the pain, we can become something so much better” My thoughts were deafening, my last shred of sensible consciousness could barely be heard or even understood. “But what about our body, I don’t want to damage anything .” “No more of this self pity, no more struggle, I want to live. I want to progress, we can do anything we want. it’s all in the mind; just let go, and you can be anything!”
Retrospect
A part of me wanted to see my psychiatrist to tell him more about what’s happening to me and try to explain as best I could. These mood shifts caused so much confusion, something I did not want to admit. I felt ashamed; I felt like a child, incompetent to my own existence. Words would come out of me like a newborn calf, and the narrative would struggle to stand, trying to make sense of the gravity of existence. Who exactly am I? Was I conceived by my own disease? Memories of when I was a younger teen popped into my head. The sleepless nights awake in bed, people concerned about my change in behavior, mixed in with periods of normalcy.
I wish that I could tell you all that I did just that, that I went to see my psychiatrist after this incident, but I didn’t. It took me a year before I could finally tell my psychiatrist about what was happening to me. And I Eventually got diagnosed and prescribed medication for my bipolar disorder, which has helped, but I want to focus on breaking down my anecdotal story to better understand the relationship Ashwagandha has with bipolar disorder, as well as giving a scientific breakdown of the perceived self concept of a bipolar disorder sufferer.
Ashwagandha’s Possible Effect On Bipolar Inflammation
The pathology of bipolar disorder is still not fully understood. But one thing is certain: studies on bipolar disorder have revealed pro-inflammatory states in depressed, manic, and euthymic states. Not only that, but individuals with bipolar disorder have a high rates of immunological dysregulatory diseases [3]. This could explain why I had periodic joint pain even when I was at a healthy weight. You might be wondering, “Why is a mental disorder, which is commonly thought to be a non-physical disorder, increasing inflammation in the body?” Could the origins of this ailment be physical rather than mental? It is too early to determine because there are contradicting data; it is possible that bipolar disorder has an inflammatory phenotype, but further research is required. As for finding a way to possibly combat this nasty inflammation problem, Ashwagandha has been shown to produce significant immunomodulatory effects by reducing IL-6 and tnf-a [4] in studies done on mice who had induced SLE (Systemic Lupus Erythematosus), a multifactorial autoimmune disorder characterized by inflammation in the joints.
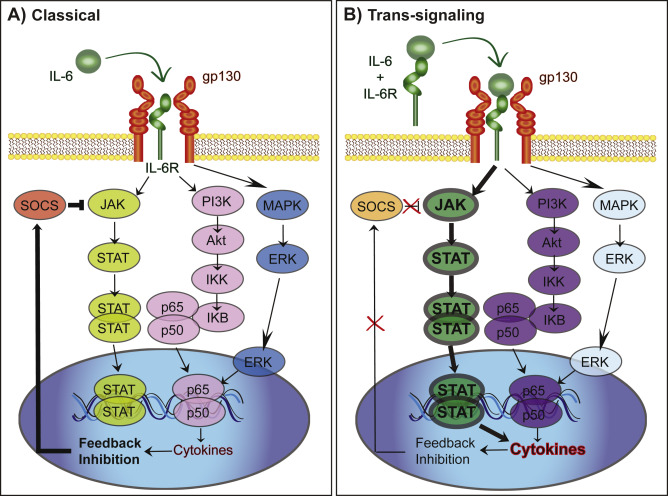
Both IL-6 and TNF-a are inflammatory cytokines. Cytokines are crucial signaling proteins that are responsible for pro- and anti-inflammatory signaling and are essential to the immune system when correctly controlled. Inflammatory cytokine overexpression, such as IL-6 (interleukin-6), has been associated to depression and anxiety disorders [5]. Furthermore, IL-6 is a target cytokine for the treatment of rheumatoid arthritis [6]. So, what are the cytokines expressed in this suggested bipolar disorder inflammatory phenotype? According to a study on cytokines and the neuroprogression of bipolar illness [7], transcriptomic (the study of all RNA molecules in a cell) modifications suggest that monocytes have an overexpression of mRNA cytokines such as TNF-, IL-1, IL-6, and CCL2. In summary, Ashwagandha has been demonstrated to alter tnf-a and IL-6, two proinflammatory cytokines that have been linked to bipolar disorder.
Bipolar Disorder And The Divided Self
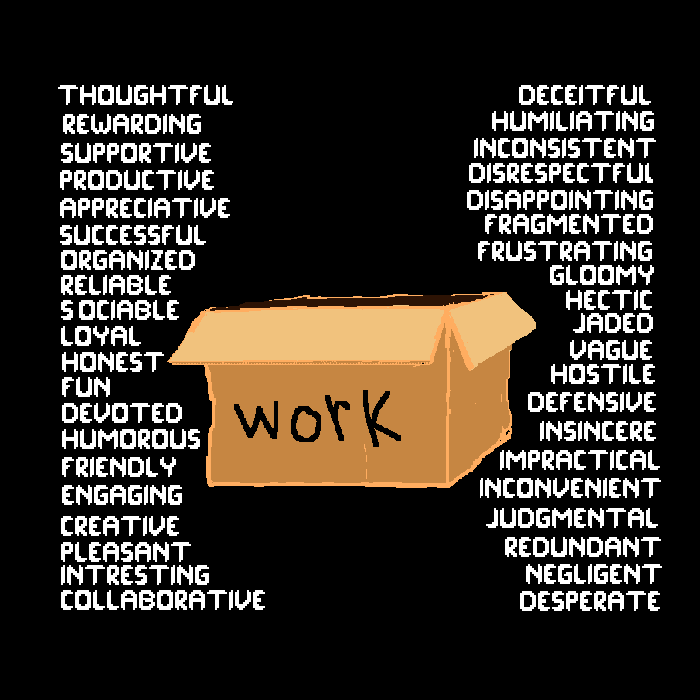
Having bipolar disorder is a confusing mess. Actually, having any mental illness is a confusing mess considering the amount of overlap and similarities many mental illnesses have with each other. But anyhow, let’s see. We have manic and /hypomanic, depressive, euthymic, and mixed episodes. These are the different states of being for a person suffering from bipolar disorder. Shifting through these states causes changes in the perception of the self, causing contradiction and a fractured sense of self. Researchers ([8] [9] ) have noticed that patients with mood disorders, like bipolar disorder, use what is called “compartmentalization” as a defense mechanism. Compartmentalization is characterized by separating incompatible cognitions. This can be positive and/or negative compartmentalization. You can think of compartmentalization as a series of boxes. Let’s say you label one of these boxes “work.” You are then given 40 adjectives, 20 positive and 20 negative, to describe work. If you were to use only negative adjectives to describe your work, that would be called negative compartmentalization. Compartmentalization is not exclusive to mental illness, it is something that every healthy person does to a certain extent, but if you have bipolar disorder, compartmentalization is usually taken to the extreme because of the nature of the disease. Looking at yourself as completely negative or completely positive makes getting a diagnosis a lot more complicated for both the sufferer and the doctor, as the sufferer is unable to “find” his true self.
What I find very interesting is a term called “splitting,” a term used to describe a patient’s mode of thinking in borderline personality disorder. Compartmentalization and splitting are two very similar terms, but used in very different connotations. You won’t find articles on bipolar disorder talking about “splitting,” because that term is often associated with personality disorders and not mood disorders. They are both defense mechanisms meant to protect the sense of self by separating incompatible cognitions. So what separates them?
Splitting is compartmentalization, but compartmentalization is not splitting. Splitting means a high level of compartmentalization, so why not label bipolar patients as splitting since often we find that patients, in fact, have a high level of compartmentalization. Well, this is because of the historical background of the word “splitting,” which has its roots in a non biological Freudian-inspired theory created by William Ronald Dodds Fairbairn called Fairbairn’s theory of attachment. The gist of the theory is that neglect in early life plays an important role in the manifestation of personality disorders, but the theory does not go into detail when it comes to the biological functions, putting more of an emphasis on the psychosocial effects and psychosocial pathology of personality disorders. So splitting is used in BPD and not bipolar disorder because splitting refers to compartmentalization as a defense against rejection:
In short, same defense mechanism, but the use/reasons as to why these defenses are “deployed” by the psyche are in fact different. This overlap in symptoms often causes confusion when trying to diagnose patients. It can take 5–10 years before a patient is diagnosed [11] with bipolar disorder. Patients are often misdiagnosed with bpd, unipolar depression, adhd, and more before they are diagnosed with bipolar disorder.
Bipolar Disorder Most Common Comorbidities And How Ashwagandha Can Help
Comorbidity means having more than one disorder, whether mental or physical. And let me tell you, bipolar disorder has a reputation for being entrenched in a slew of psychiatric disorders[12]. In other words, you are statistically more likely to suffer from more than one medical condition if you have bipolar disorder. Here are some common psychiatric comorbidities.
- Anxiety Disorders
- panic disorders
- social anxiety disorder
- personality disorders
Bipolar disorder has quite a few medical comorbidities as well.
- diabetes mellitus
- chronic pulmonary disease
- migraines
- substance use disorder
- autoimmune diseases
(Disorders highlighted in green are those that have the potential for Ashwagandha to have a therapeutic effect on. Ashwagandha is not intended to treat or cure any disease. It has however been shown to be anti-diabetic, anti anxiety, and anti-inflammatory, and are therefore highlighted.)
One of the reasons why I believe taking Ashwagandha can really help if you have bipolar disorder is its adaptogenic properties. Adaptogen have multi-targeted mechanisms of actions and are often used in network pharmacology for research in the hopes of finding treatments for complex diseases.
Real Talk
If you yourself have bipolar disorder, I want to make it clear that my intentions are not to freak you out into thinking you have another disease or try to scare you into thinking you need Ashwagandha. My intentions are to equip you with knowledge that could help you in your journey. I myself have suffered from panic and anxiety disorders, which devolved into obsessive thoughts and agoraphobia when I was around 17, before I was diagnosed with bipolar disorder. I went to therapy when I was around 18 and realized my unhealthy coping mechanism of escapism. But knowing and identifying your unhealthy habits is a fraction of the battle. For me, the hardest part was asking for help. I would much rather take my chances by self medicating with various substances, trying to keep myself from falling back down into the abyss of a depressive episode. The journey towards a bipolar diagnosis is a confusing one. Some may never even reach their diagnosis, stuck in limbo, a slave to their own disease. I hate the thought of someone having to go through that because in a sense, I was that person stuck in limbo; even after my diagnosis, I didn’t fully accept it. I found myself in Denial, “I’m fine” I would tell myself. “I was just being dramatic, and I have changed; I don’t need medication.”
You can lead a horse to water, but you can’t force a horse to drink, no matter how dehydrated or sick it may be. I mean, who would want to admit to having a chronic lifetime disease and the stigma that comes with it. No, what our mind wants is a rosy, pink, sugar-coated lens to look at ourselves through. So we sometimes find ourselves separating the wheat from the chaff, so to speak, removing all the bad and taking all the good and running… Running as fast as we can, we don’t dare to stop, for if we do, we will fall into a pit of despair. So we don’t want to think. Just keep going; Hedonism will be your guide; do what makes you happy.
Oh, the different paths our diseased mind takes us, how inconspicuous it looks to the inexperienced bullshi**er. Every bipolar patient has their own triggers for mania and/or hypomania, and it is in those episodes that we find ourselves feeling “invincible.” I don’t have a problem. If I did have a problem, why do I feel so good, like I can take on the world? Okay, sure, you’re right, “sick” people don’t feel that good. I imagine you have an idea of what “sick” means. I imagine you are most likely labeling the depressive episodes as sick and the manic or hypomanic episodes as a “healthy” state, but do you think it is going to be sustainable? No, I have seen this play out too many times before, both in my own life and in other people’s lives. “There is a price tag hanging off having all that fun”, what comes up must come back down, there are no free meals in life. Pick your poison of proverbs and expressions and accept the reality of having bipolar disorder for what it is: a dichotomy of mania/hypomania and depression and everything in between. An ever-changing, uncontrollable force of nature that cannot be conquered on your own.
Denial
Denial, how dangerous and destructive this defense mechanism can be for the bipolar patient. There is a hierarchy when it comes to defense mechanisms, 7 levels descending into madness.
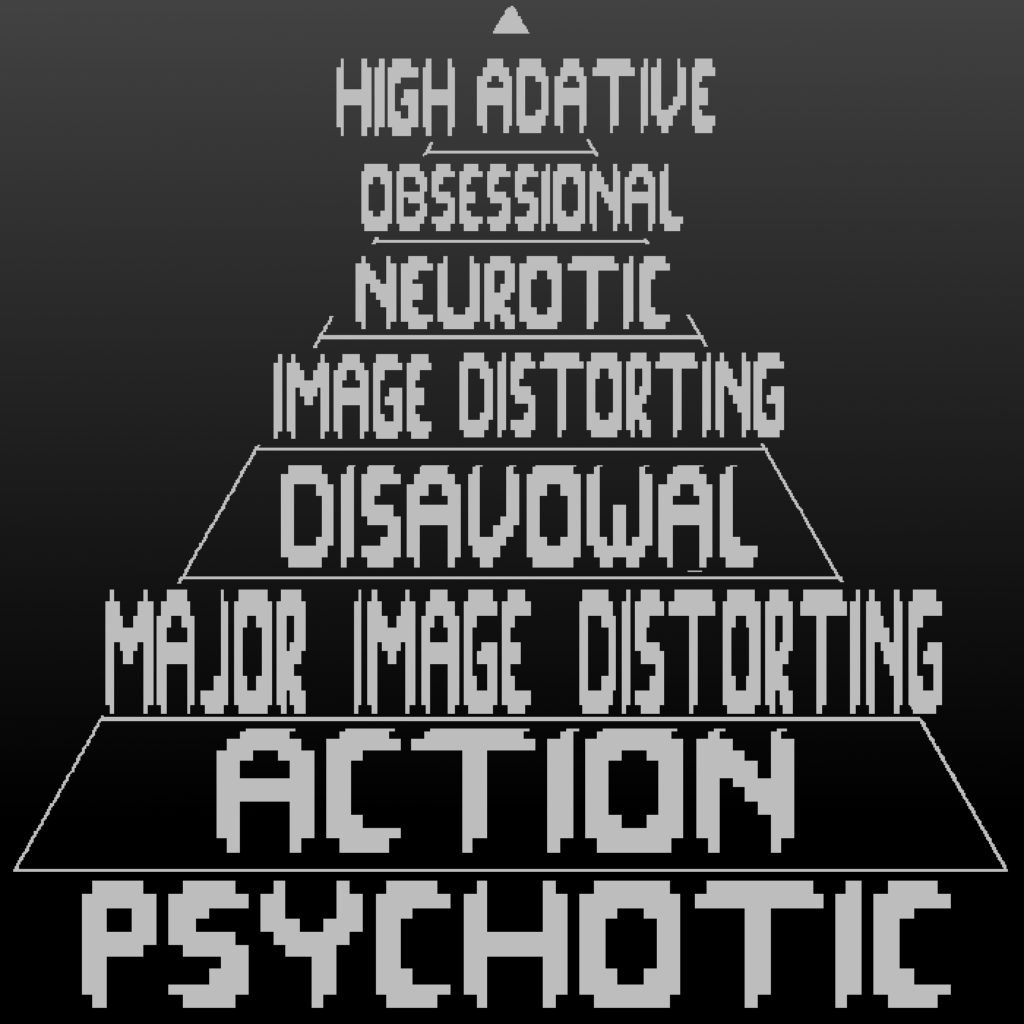
This example that I am going to show you guys is from a study done on identifying psychotic defense mechanisms (level 0) in clinical interviews.
“Example 1. Patient A is a 34-year-old female diagnosed with bipolar disorder and followed
at an outpatient clinic, a specialized section for patients with personality and mood disorders. The patient explains that she was recently hospitalized for a depressive episode with continual suicidal thoughts. Before being hospitalized, she would hide crying at home and not tell her husband anything about it. She reports that her husband often became nervous with her and reproached her for not tidying their home well enough before he returned from work in the evening. She stated that she could not tell her husband about what she feels.
Therapist: What makes it so difficult for you to talk to him?
Patient: It stresses me. You, I know that you are not part of my family. You are not going to judge me. I can tell you, but I cannot tell my family.
T: What makes it difficult for you to talk to your family?
P: Well, there is no reason for me to be depressed. I have everything I need. Things are fine with my husband, and with my children. I have a house and they all like me, so things are fine [psychotic denial].
Later on in the interview, the patient reports that she sometimes gets nervous with her children (a 4-year-old girl and an 8-year-old boy) because they do not tidy up their toys. If she has to take care of both of them, she feels overwhelmed. So she has organized an alternate day care for each of them to stay with one at a time.
P: With my son, I get tired quickly. I give him handicrafts, I begin to do them with him and then I leave. So he tells me that I never do anything with him and that hurts.
T: It hurts?
P: Yes. I would like to do more things with him, but I am not able to. With my daughter things are easier, she does not need me [psychotic denial].
In this transcript, the patient reports that she cannot talk to either her husband or her family about her difficulties. When the interviewer tries to clarify what prevents her from doing so, she suddenly refuses to acknowledge some aspects of the reality of her experience (“I have no reason to be depressed”) and some aspects of the external reality (“things are fine with my husband and with my children”; “a 4-year-old child does not need her mother”).
For the patient, talking about these difficulties and having to remember them to be able to think about them triggers so much anxiety that the only recourse is to deny the existence of the stressor involved. This defense is psychotic denial, which differs from minor denial (which concerns only internal reality) in the way that it regards both internal and external reality. It implies that some aspects of the reality are kept out of consciousness. It can be about an entire part of life (pregnancy denial, death denial) or about more limited aspects (as in the present example).”[13]
Denial affects the way you speak about yourself to others, and it also causes an internal pathology by not accepting and integrating both the good and the bad. You are also more likely to skip out on your medications, which is referred to as non adherence. A study done on coping and medication adherence in bipolar patients saw a strong correlation between acceptance and medication adherence and a strong correlation between denial and non adherence to medication. In other words, if you accept your disease, you are more likely to continue taking your medication; if you deny it, you will most likely stop taking your medication and “relapse” into mania or hypomania. Over 40% of bipolar patients [14] skip out on their medication.
Conclusion
So how do we begin to integrate ourselves if we find ourselves lost? We must construct “bridges” to fill the gaps in our minds. Orient yourself through speech and/or writing, to be willing to play the long game and take the blinders of impulsivity off. Remember to breathe and to find something to anchor yourself to reality when your thoughts are racing towards destruction. This is easier said than done, and you will not be able to do it alone. With medicine, complementary medicines like Ashwagandha, therapy, and self-improvement, you can orient yourself towards something greater.
I have to say learning about one’s own illness can be very terrifying but necessary to getting better. Learning about your shortcomings, dealing with the guilt and denial that can come with mental illness. I don’t envy myself or others who struggle with their mental health. Trendy it may be to bare your scars and parade yourself as a walking billboard of oppression. I find it vital to work on yourself and try not to be a slave to your own disease.
Ashwagandha has been of great help to me, and I believe it is worth a try. If you decide to try Ashwagandha for yourself, I would recommend starting on ksm-66 and then trying the others if you feel like you need something stronger. I myself have been taking Ashwagandha for 4 years off and on and have recently made the switch to using Shoden for the past year or so, and it has been working great for me. Shoden is the most bioavailable Ashwagandha on the market, and I have a page going into more detail on it if you are more interested.